

The U.S. is getting worse at allocating organs
New evidence of an old problem


Suppose a patient in his twenties is brought to a hospital following a motorcycle crash.1 The doctors can’t save him, but he had consented to being an organ donor, so the organ recovery team removes the viable organs following his death. This raises a question: Who should get these organs?
This is a hard problem. Part of the issue is that there are a lot of people who need them. As of March 13th, 2025, there are 104,462 people in the United States waiting for a lifesaving organ, with the vast majority—around 90,000 people—in need of a kidney. Around one in seven Americans have chronic kidney disease. (In Canada, the number is one in ten.) In 2023, there were only 27,332 kidney transplants, which means that, every year, tens of thousands of Americans either stay on dialysis or die waiting for a transplant. Since there aren’t enough to go around, we have to figure out who gets the ones that become available.
Another problem is that you can’t put any old organ into a different body. The blood types have to be compatible, as do the human leukocyte antigens, plus some other stuff. But there’s also just the basic size of the organ. A transplant surgeon once told me a particular transplant would lead to too much “bouncing around.” There are better and worse matches, and while doctors want the best match possible, some wiggle room is possible.
Then there’s the problem of viability. A kidney is only viable outside the body for up to forty-eight hours. This is better than hearts and lungs, which are only good for four to six hours (though a new technology, ex vivo organ perfusion, is extending that timeframe).
All of this means that there is, at most, forty-eight hours to find the patient out of the 90,000 who is the best match, get the organ to him or her, and do the transplant so that it doesn’t go to waste. (In the case of our motorcyclist, he might have provided multiple organs, so the problem is even more complex.) America’s a big place, so geography plays a role. You can courier an organ for a surgery, but that takes more time, increases the risk that it will be delayed, or, in one 2018 heart’s case, mistakenly left on a plane.
But we also have to do some ethics. There’s broad agreement among ethicists and the general public that organs shouldn’t be provided on a first come, first served basis or given to the highest bidder. How long someone has been waiting is a factor, but, all else equal, sicker people should get priority. While dialysis can extend a person’s life for years in some cases, some people become intolerant to it, which means they need a new kidney immediately. We want to get the organ to the right person, where ‘right person’ means not just the patient with the right bodily features, but also the one who needs it most. And we need to do this fast.
Do you want to be fast or fair?
The organ allocation process is an excellent example of the tradeoff between fairness and efficiency. We want the organs to go to the people who deserve them most, but the quest for fairness can’t come at the expense of actually transplanting organs. If it takes too long to figure out who’s most deserving, it would be better to give the organ to someone who will benefit, even if it means that the more-deserving person misses out.
But the problem can go the other way too. Someone might reason that any transplant is better than nothing, then decide to give the organ to whoever’s a good match, regardless of where they are in the line.
It turns out that this latter problem has been occurring across the United States in recent years, which we know due to some excellent reporting from Brian M. Rosenthal, Mark Hansen, and Jeremy White at the New York Times. According to their reporting,
officials regularly ignore the rankings, leapfrogging over hundreds or even thousands of people when they give out kidneys, livers, lungs and hearts. These organs often go to recipients who are not as sick, have not been waiting nearly as long and, in some cases, are not on the list at all, a New York Times investigation found.
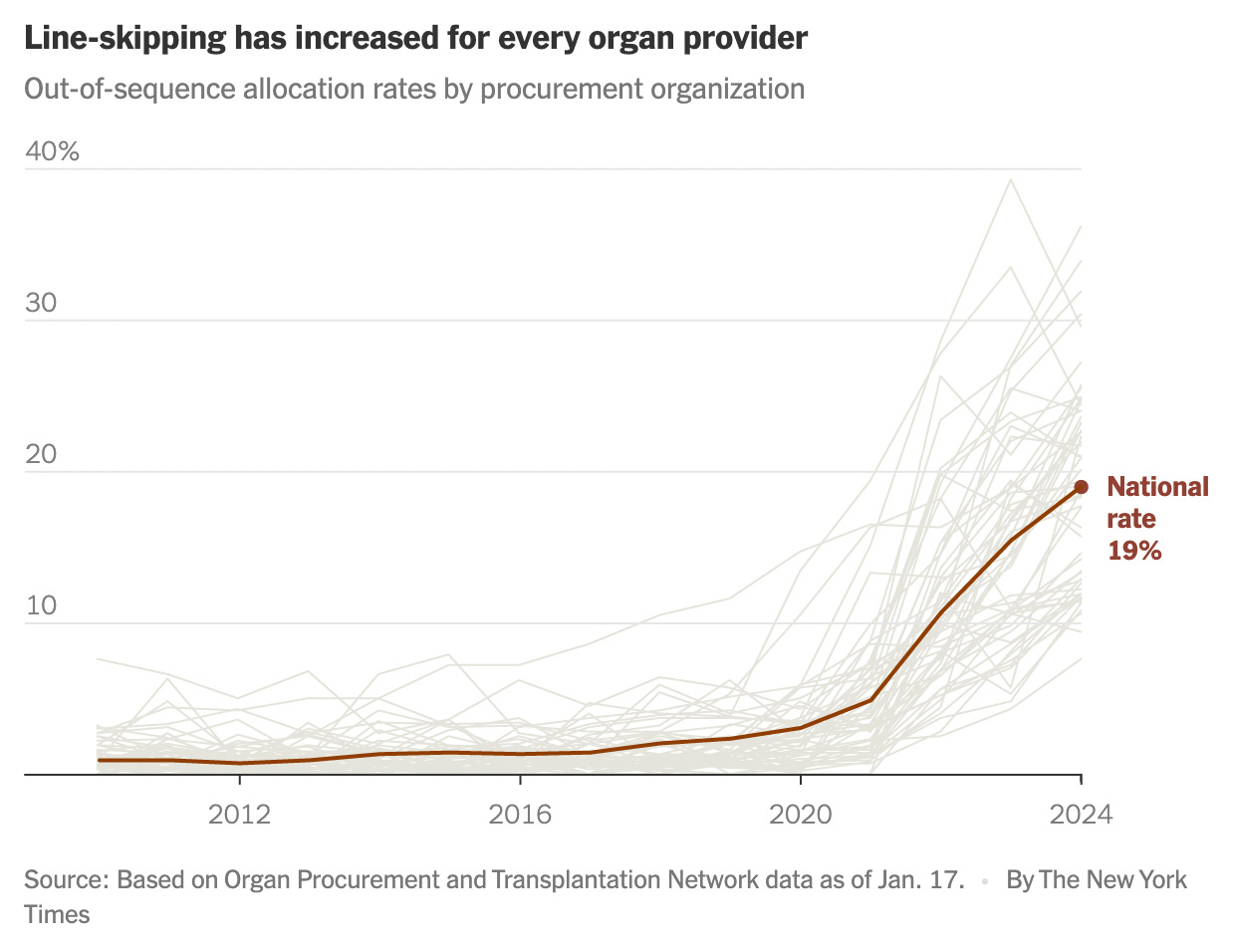
Last year, officials skipped patients on the waiting lists for nearly 20 percent of transplants from deceased donors, six times as often as a few years earlier. It is a profound shift in the transplant system, whose promise of equality has become increasingly warped by expediency and favoritism.
In the United States, nonprofits are given government contracts to distribute organs for a region. Some cover a state, but some more-populous states have multiple organizations (California, for instance, has four). These organ procurement organizations decide where the organs go and who gets priority. (In contrast, in Canada, each province has its own government-affiliated organization. Ontario’s Trillium Gift of Life Network is part of Ontario Health, for example. The exception is Canadian Blood Services, which is an independent nonprofit that helps coordinate transplants between provinces.)
The basic process for the U.S. organ procurement organizations is that, when an organ becomes available, the OPO has an algorithm to determine the patients who, out of the entire list, are matches for the organ. The OPO is supposed to offer the organ to the doctor responsible for the patient at the top of this new list.2
The algorithm isn’t perfect, so the patient first in line might not actually be a good fit. In that case, the OPO will offer it to the first patient’s doctor, who will decline it, so then the organ is supposed to go to the second patient in line, wait for that doctor to accept or decline, and so on.
Transplant surgeons are aware that time is of the essence, so this isn’t done by email or a call to the front desk. There’s a transplant coordinator who, when contacted about an organ, will very quickly confer with the surgeon. But even this takes time, and it might take the OPO multiple tries before someone accepts the organ. And so you can imagine the stress of the OPO person sitting there, trying to get rid of an extremely valuable kidney, but no one’s taking it.
Although fairness requires that the OPO continues down the list until a doctor accepts, OPOs are allowed to expedite the process by using what’s called an open offer. In these cases, instead of finding the top patient, the OPO offers the organ to a hospital, which can then give the organ to any of its patients. Hospitals with a transplant center are almost certainly going to have a patient who’s a good-enough match, so the organ is now easy to give away. This is good, but the problem is that the hospital’s patients might not be anywhere near the top of the list, which means using an open offer results in queue jumping. (To be clear, the patient receiving the organ won’t know this is the case.) In some cases reported by the Times, the person who got the organ was thousands of spots down and patients in the top-ten weren’t even given a chance.
As the Times’s data shows, for years, the rate of open offers was two percent. But, starting around 2020, open offers increased. The national average is now nineteen percent.
The reasons for this change are complex, but a driving factor was pressure from various levels of government to reduce the number of wasted organs (i.e., organs that aren’t transplanted in time). In 2020, the ‘discard rate’ was around eighteen percent.
As I said, there’s a real tradeoff here between fairness and efficiency. Suppose OPOs could place every organ by doing away with considerations of fairness. It would be fast but unfair. As they add more fairness, at some point, the discard rate will go up. The question then becomes how much waste we’re willing to accept for the sake of fairness. There’s no fact of the matter here—whether a loss of eighteen percent is acceptable or not is a value judgment, and people will disagree about how acceptable that is—but it was reasonable for the government to demand improvement.
The problem is that, as open offers increased, so did waste. It got worse! In their quest to reduce waste, the OPOs managed to increase waste and decrease fairness. Here’s a chart from the Times article:

The Times’s investigation shows that there’s more going on than simply pursuing efficiency, including OPOs giving seemingly unjustified preferential treatment to some transplant centers. The article doesn’t explain why the rate of wasted organs has been increasing, and the chart above shows that the discard rate started climbing before 2020, but this is still on the OPOs.
More OOPs than OPOs
In the broader context of criticisms of America’s organ allocation system, none of this is surprising. In 2023, President Biden signed a bipartisan bill that would allow for changes to the transplant system (here’s the full text). In the crosshairs was the United Network for Organ Sharing, or UNOS, a nonprofit that has run federal organ procurement and distribution for over forty years. UNOS has been criticized for years for mishandling the allocation process, including the literal mishandling of misplaced organs. It was also the focus of a Senate Finance Committee investigation in 2022, which found significant shortcomings with its processes.
But reform attempts go back further. In his first term, President Trump signed an executive order called “Advancing American Kidney Health”. It was also under Trump that Congress added pressure on OPOs to improve or lose their funding.
Biden’s bill changed how the Health Resources and Services Administration manages the organ allocation process. The HRSA is an agency of the U.S. Department of Health and Human Services, which is now run by Robert F. Kennedy, Jr. So far, it’s unclear how Trump’s broader changes to HHS will affect organ allocation. What’s clear is that the system isn’t working. Broad reform is needed, as are the right kinds of oversight. As the Times article shows, Trump’s first attempt to improve OPOs only made the outcomes worse. But maybe now, after years of pressure, improvement is coming.
The rumors are true that riding a motorcycle increases your risk of becoming a deceased organ donor. According to one study, “from 2005 to 2021, there were 21% more organ donors and 26% more transplant recipients per day during motorcycle rallies in regions near those rallies compared with the four weeks before and after the rallies.”
Often, the transplant team doing the recovery will alert the OPO ahead of time that an organ or organs will soon be available, which buys the system more time. Even when a patient is legally dead by neurological criteria, it’s not uncommon for the transplant team to keep the body on a ventilator or other ‘life support’ to preserve the organs while they identify a recipient. This is what happened when the actress Anne Heche died.
When supply of kidneys is only 30 percent of the need and a transplantable kidney has a short useful life there will be real problems with both fairness in allocation and waste of untransplanted kidneys. What is not clear is WHY the problems of fairness of allocation and waste are both getting worse. Is it because of the Biden and Trump laws or in spite of these laws?